


In a medical breakthrough that pushes the boundaries of human survival, a 33-year-old man has been kept alive for a remarkable 48 hours without any lungs, a feat previously considered impossible. Surgeons at Northwestern University successfully removed the patient’s severely infected lungs and utilized an advanced "artificial lung" system to sustain him until a life-saving double lung transplant could be performed. This pioneering case, detailed in the latest issue of the Cell Press journal Med, offers a beacon of hope for critically ill patients awaiting organ donations and provides crucial new insights into the reversibility of severe lung damage.
A Race Against Time: Acute Respiratory Distress Syndrome and Organ Failure
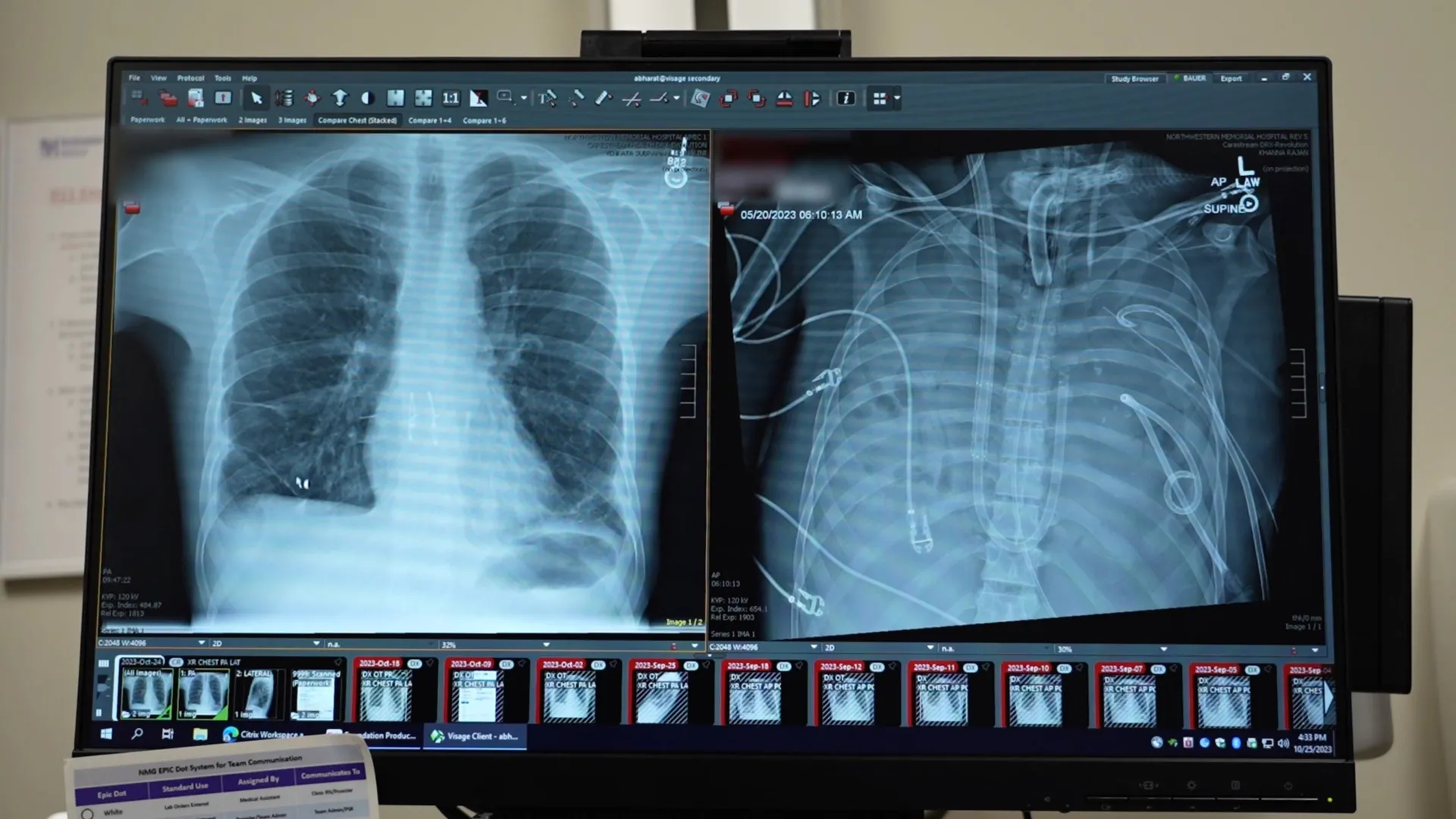
The patient’s critical condition began with a severe case of influenza, which rapidly escalated into a life-threatening bacterial pneumonia. This aggressive infection triggered acute respiratory distress syndrome (ARDS), a condition characterized by widespread inflammation and fluid accumulation in the lungs, severely impairing their ability to transfer oxygen to the bloodstream. As ARDS took hold, the patient’s lungs became irrecoverably damaged, a state that typically leads to a rapid and fatal decline.
"He was critically ill. His heart stopped as soon as he arrived. We had to perform CPR," stated lead author Ankit Bharat, a thoracic surgeon at Northwestern University, recounting the harrowing initial moments of the patient’s admission. "When the infection is so severe that the lungs are melting, they’re irrecoverably damaged. That’s when patients die."
The cascading failure extended beyond his respiratory system; his heart and kidneys began to falter under the immense strain. At this critical juncture, with his native lungs beyond repair and his overall health deteriorating, a double lung transplant emerged as his sole chance of survival.
The Unthinkable Decision: Removing Diseased Lungs to Halt Infection
The patient’s lungs were not merely non-functional; they were actively contributing to the lethal spread of infection throughout his body. However, his physiological state was too precarious to immediately undergo the complex and demanding procedure of a double lung transplant. The surgical team faced an unprecedented challenge: how to keep a patient alive when the very organs responsible for breathing and vital gas exchange had to be removed, and a replacement was not yet available.
"The heart and lungs are intrinsically connected," Dr. Bharat explained. "When there are no lungs, how do you keep the patient alive?"
This question propelled the development of an innovative extracorporeal membrane oxygenation (ECMO) system, specifically adapted to function as an "artificial lung." This sophisticated apparatus was designed to temporarily assume the critical functions of the patient’s native lungs. It meticulously oxygenated his blood, efficiently removed carbon dioxide, and crucially, provided circulatory support. This allowed his heart and other vital organs to continue functioning, creating a vital window of opportunity for recovery and transplant.
The Artificial Lung as a Lifeline: A 48-Hour Bridge to Transplant
Following the radical decision to remove the diseased lungs, the patient’s condition began to show signs of stabilization. The artificial lung system effectively managed his oxygenation and carbon dioxide levels, alleviating the immense pressure on his cardiovascular system. As a result, his blood pressure normalized, his failing organs began to show signs of recovery, and the rampant infection started to recede.
The critical 48-hour period was a testament to the efficacy of the artificial lung system. During this time, the medical team meticulously monitored the patient’s vital signs, managed his infection, and prepared for the eventual transplant. The availability of donor lungs, often a significant hurdle in transplant medicine, arrived at the opportune moment.
"The patient’s condition improved significantly," Dr. Bharat noted. "His blood pressure stabilized, his organs started recovering, and the infection came under control."
Two days after the removal of his native lungs and the implementation of the artificial lung, donor lungs became available. The surgical team, now working with a more stable patient, successfully executed a complex double lung transplant. The long-term prognosis for the patient has been overwhelmingly positive. More than two years following the procedure, he is reportedly living a normal life, with healthy and fully functional transplanted lungs.
Challenging Conventional Wisdom: New Evidence on Irreversible Lung Damage
This groundbreaking case challenges long-held assumptions within the medical community regarding the management of severe ARDS. Traditionally, lung transplantation has been primarily reserved for patients suffering from chronic, progressive lung diseases such as interstitial lung disease or cystic fibrosis, where gradual deterioration necessitates a replacement. The prevailing approach for acute ARDS, even in its most severe forms, has been supportive care, with the hope that the lungs might eventually recover.
"Conventionally, lung transplant is reserved for patients who have chronic conditions like interstitial lung disease or cystic fibrosis," Dr. Bharat commented. "Currently, people think if you get severe ARDS, you keep supporting them and ultimately the lungs will get better."
However, the detailed examination of the patient’s explanted lungs provided compelling new evidence. Molecular analysis revealed extensive and irreversible scarring, coupled with significant damage to the immune system within the lung tissue. These findings unequivocally indicated that the lungs were beyond any possibility of functional recovery.
"For the first time, biologically, we are giving molecular proof that some patients will need a double lung transplant, otherwise they will not survive," Dr. Bharat asserted. This scientific validation underscores the critical need to re-evaluate treatment protocols for severe ARDS and to consider lung transplantation as a viable and potentially life-saving option in acute settings, not just chronic ones.
A Potential Lifesaving Bridge: Implications for Future Transplant Medicine
The implications of this case extend far beyond the individual patient. The successful implementation of an artificial lung system as a bridge to transplant represents a significant advancement in extracorporeal life support technology and organ transplantation strategies. It demonstrates that it is possible to maintain life and support organ function for an extended period even in the complete absence of native lungs.
While the current approach is highly specialized, requiring advanced expertise, infrastructure, and dedicated teams, Dr. Bharat expressed optimism about its future broader application. He envisions the development of more standardized and accessible artificial lung systems that can be deployed in a wider range of medical centers. This could dramatically improve the chances of survival for critically ill patients who are currently at the mercy of their failing lungs and the availability of donor organs.
"In my practice, young patients die almost every week because no one realized that transplantation was an option," Dr. Bharat lamented. This sentiment highlights a critical gap in awareness and timely intervention. He emphasized that for severe lung damage caused by respiratory viruses or infections, even in acute settings, a lung transplant can be a definitive, life-saving intervention.
The development and validation of this artificial lung system offer a new paradigm for managing patients with catastrophic lung injury. It suggests that the traditional dichotomy between supportive care for ARDS and transplantation may need to be re-examined, with a more integrated approach that readily considers transplantation as a primary treatment option in specific, severe cases.
Broader Impact and Future Directions
The success of this pioneering case is likely to spur further research and development in artificial organ technologies. The ability to sustain a patient for 48 hours without lungs not only highlights the ingenuity of the medical team but also the rapidly advancing capabilities of extracorporeal life support. This technology could potentially be adapted for other organ failures, further expanding the possibilities for life support.
Furthermore, the molecular evidence obtained from the removed lungs could inform the development of new diagnostic tools and prognostic indicators for ARDS. Identifying patients who are unlikely to recover their lung function could lead to earlier and more definitive treatment decisions, including timely referral for transplantation.
The case also brings into sharper focus the ongoing need for organ donors. While technological advancements can extend life and bridge critical gaps, the ultimate solution for many organ failures remains transplantation. Public awareness campaigns and policies aimed at increasing organ donation rates are crucial to ensure that such life-saving interventions are available to all who need them.
In conclusion, this remarkable medical achievement represents a significant leap forward in critical care and transplant medicine. By demonstrating the feasibility of prolonged survival without lungs, supported by an artificial lung system, the Northwestern University team has not only saved a patient’s life but has also paved the way for a future where severe lung damage may no longer be an insurmountable obstacle to survival. The research published in Med is poised to influence clinical practice and inspire further innovation in the pursuit of saving lives.